
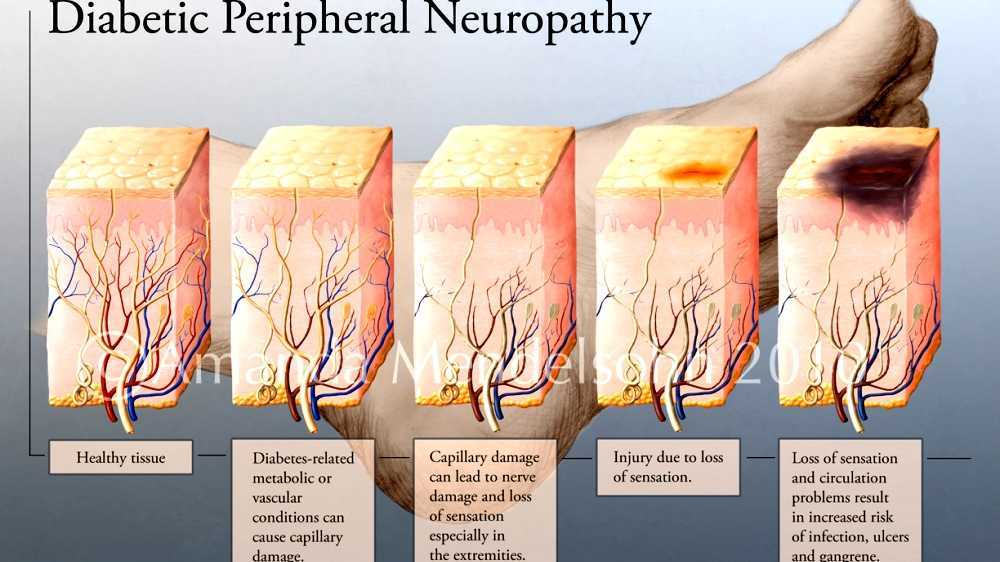
Diabetic neuropathy is a nerve damage disorder associated with diabetes mellitus. This condition is thought to be caused by a diabetic microvascular injury involving small blood vessels supplying the nerve (vasa nervorum) in addition to the macrovascular conditions that can accumulate in diabetic neuropathy. The relatively common conditions that may be associated with diabetic neuropathy include third, fourth, or sixth cranial nerve palsies; mononeuropathy; mononeuropathy multiplex; amyotrophy diabetes; painful polyneuropathy; autonomic neuropathy; and thoracoabdominal neuropathy.
Video Diabetic neuropathy
Signs and symptoms
Diabetic neuropathy affects all peripheral nerves including sensory neurons, motor neurons, but rarely affects the autonomic nervous system. Therefore, diabetic neuropathy can affect all organs and systems, as they are all reserved. There are several different syndromes based on organ systems and affected members, but this is by no means exclusive. A patient can have sensorimotor and autonomic or other combination neuropathy. The signs and symptoms vary depending on the affected nerve (s) and may include symptoms other than those listed. Symptoms usually develop gradually over the years.
Symptoms may include the following:
- Difficulty with balance
- Numbness and tingling extremities
- Dysesthesia (abnormal sensation to body part)
- Diarrhea
- Erectile dysfunction
- Urinary incontinence (loss of bladder control)
- Face, mouth and eyelid sagging
- Vision changes
- Dizzy
- Muscle weakness
- Difficulty swallowing
- Speech interruption
- Fasciculation (muscle contraction)
- Anorgasmia
- Retrograde ejaculation (in men)
- Burns or electricity
Maps Diabetic neuropathy
Pathogenesis
The following factors are thought to be involved in the development of diabetic neuropathy:
Microvascular disease
Vascular and neurological disease is closely related and intertwined. The blood vessels depend on normal nerve function, and the nerves depend on adequate blood flow. The first pathological changes in small blood vessels narrow the blood vessels. As the disease progresses, neuronal dysfunction is closely correlated with the development of vascular abnormalities, such as thickening of the capillary basement membrane and endothelial hyperplasia, which contribute to reduced oxygen and hypoxic pressures. Neuronal ischemia is an obvious characteristic of diabetic neuropathy. Vascular opening agents (eg, ACE inhibitors, 1-antagonists) may cause substantial improvements in neuronal blood flow, with an appropriate increase in the speed of nerve conduction. Thus, small blood vessel dysfunction occurs early in diabetes, parallel to the development of neural dysfunction, and may be sufficient to support the severity of structural, functional, and clinical changes observed in diabetic neuropathy.
Sophisticated advanced end products
Increased glucose levels in cells lead to non-enzymatic covalent bonds with proteins, which alter their structure and inhibit their function. Some glycosylated proteins have been implicated in the pathology of diabetic neuropathy and other long-term diabetes complications.
Polyol Path
Also called the sorbitol/aldose reductase pathway, the polyol pathway appears to be involved in diabetic complications, particularly in microvascular damage to the retina, kidneys, and nerves.
Sensorimotor polyneuropathy
The longer nerve fibers are affected to a greater extent than the shorter ones because the speed of nerve conduction is slowed in proportion to the length of the nerve. In this syndrome, a decrease in sensation and loss of reflex occurs first in the toes on each leg, then extends upwards. Usually described as a distribution of numbing socks, sensory loss, disesthesia and pain at night. The pain may feel like a burning, stinging, achy or dull sensation. Pin and needle sensations are common. The loss of proprioception, the sense in which the limbs are in outer space, is affected early on. These patients can not feel when they step on a foreign object, like flakes, or when they develop porous from inappropriate shoes. As a result, they are at risk of developing ulcers and infections of the feet and legs, which can lead to amputations. Similarly, these patients may get some knee, ankle or leg fractures, and develop a Charcot joint. Loss of motor function produces dorsiflexion, toe contraction, loss of interosseal muscle function causing contraction of the fingers, called hammer legs. This contracture occurs not only in the legs but also in the hands where muscle loss makes the hands look thin and skeletal. Loss of muscle function is progressive.
Autonomic neuropathy
The autonomic nervous system consists of the nerves serving the heart, lungs, blood vessels, bones, adipose tissue, sweat glands, digestive system and genitourinary system. Autonomic neuropathy can affect one of these organ systems. The most commonly recognized autonomic dysfunction in diabetics is orthostatic hypotension, or becomes dizzy and may faint when standing because of a sudden drop in blood pressure. In the case of autonomic diabetic neuropathy, it is due to heart and arterial failure to fit precisely the heart rate and blood vessel tone to keep the blood constantly and flowing completely to the brain. These symptoms are usually accompanied by loss of respiratory sinus arrhythmias - a normal change in heart rate seen with normal breathing. These two findings suggest autonomic neuropathy.
Manifestations of the gastrointestinal tract include gastroparesis, nausea, bloating, and diarrhea. Because many diabetics take oral medication for their diabetes, the absorption of these drugs is strongly influenced by delayed gastric emptying. This can lead to hypoglycemia when oral diabetes agents are taken before meals and are not absorbed for hours, or sometimes days later when there is already normal or low blood sugar. Slow movements of the small intestine can cause bacterial overgrowth, exacerbated by the presence of hyperglycemia. It causes bloating, gas and diarrhea.
Urinary symptoms include urinary frequency, urgency, incontinence and retention. Again, because urinary retention, urinary tract infections are common. Urinary retention may cause bladder diverticula, stones, reflux nephropathy.
Cranial neuropathy
When the cranial nerve is affected, the oculomotor nerve neuropathy (cranial nerve # 3) is the most common. The oculomotor nerve controls all the muscles that move the eye except the lateral rectum and superior tilt muscles. It also serves to narrow the pupils and open the eyelids. The onset of the third nerve palsy of diabetes is usually abrupt, starting with frontal or periorbital pain and then diplopia. All of the oculomotor muscles innervated by the third nerve may be affected, but those who control the pupil size are usually well preserved early on. This is because parasympathetic nerve fibers in CNIII affecting pupil size are found on the periphery of the nerve (in terms of cross-sectional view), which makes them less susceptible to ischemic damage (because they are closer to the vascular supply). The sixth nerve, the nerve abducens, which conserve the lateral rectus rectus muscles (moving the lateral eye), is also frequently exposed but the fourth nerve, the trolear nerve (supplying the superior oblique muscle, which moves the eye down) involvement is unusual. Mononeuropathy of the thoracic or lumbar spinal cord may occur and lead to a painful syndrome that resembles a myocardial infarction, cholecystitis or appendicitis. Diabetics have a higher incidence of trap neuropathy, such as carpal tunnel syndrome.

Diagnosis
Diabetic peripheral neuropathy is the most likely diagnosis for someone with diabetes who has pain in the legs or feet, although it may also be caused by a deficiency of vitamin B 12 or osteoarthritis. A 2010 review in the Journal of the American Medical Association's "Rational Clinical Examination Series" evaluates the usefulness of clinical examination in diagnosing diabetic peripheral neuropathy. While doctors typically assess the appearance of the foot, the presence of ulceration, and ankle reflexes, the most useful physical examination findings for large fiber neuropathy are abnormally decreased vibrational perception to a 128-Hz tuning fork (ratio possible ratio (LR), 16-35) or pressure sensation with 5.07 Semmes-Weinstein monofilament (LR range, 11-16). The normal results on vibration testing (LR range, 0.33-0.51) or monofilament (LR range, 0.09-0.54) make large fiber-peripheral neuropathy of diabetes less likely. The combination of signs does not perform better than these 2 individual findings. Neural conduction tests may indicate diminished peripheral nerve function, but are rarely correlated with the severity of peripheral neuropathy of diabetes and are not appropriate as a routine test for the condition.
Classification
Diabetic neuropathy includes a range of different neuropathic syndromes that can be ruled out in the following way:
- Focal and multifocal neuropathy:
- Mononeuropathy
- Amyotrophy, radiculopathy
- Multiple lesions "mononeuritis multiplex"
- Entrapment (eg median, ulnar, peroneal)
- Symmetrical neuropathy:
- Acute sensory
- Autonomous
- Distal symmetrical polyneuropathy (DSPN), a type of diabetes also known as diabetic peripheral neuropathy (DPN) (the most common presentation)

Prevention
Prevention is by controlling good blood sugar and exercise.

Treatment
Except for tight glucose control, treatments to reduce pain and other symptoms.
Options for pain control include antiepileptic drugs (AED), serotonin-norepinephrine reuptake inhibitors (SNRI), tricyclic antidepressants (TCAs), and capsaicin creams. About 10% of people who use capsaicin cream have great benefits.
A systematic review concluded that "traditional tricyclic and anticonvulsant antidepressants are better for relieving short-term pain than new generation anticonvulsants." Further analysis of previous studies has shown that carbamazepine, venlafaxine, duloxetine, and amitriptyline agents are more effective than placebo, but the comparative effectiveness of each agent is unclear.
The three drugs approved by the US Food and Drug Administration for diabetic peripheral neuropathy (DPN) are duloxetine antidepressants, pregabalin anticonvulsants, and opentidol long-term opentidol ER. Before attempting a systemic drug, some doctors advise to treat local peripheral neuropathy that is localized to the lidocaine patch.
Antiepileptic drugs
Some guidelines from medical organizations such as the American Association of Clinical Endocrinologists, the American Academy of Neurology, the European Society's Neurological Federation, and the National Institute of Clinical Excellence recommend AED, such as pregabalin, as first-line treatment for painful diabetic neuropathy. Pregabalin is supported by low-quality evidence as it is more effective than placebo to reduce diabetic neuropathic pain but the effect is small. Studies have reached different conclusions about whether gabapentin relieves pain more effectively than placebo. The available evidence is not enough to determine whether zonisamide or carbamazepine is effective for diabetic neuropathy. The first metabolism of carbamazepine, known as oxcarbazepine, appears to have a small beneficial effect on pain. The systematic review and meta-analysis 2014 network concluded topiramate, valproic acid, lacosamide, and lamotrigine are not effective for pain from peripheral diabetic neuropathy. The most common side effects associated with the use of AED include drowsiness, dizziness, and nausea.
Serotonin-norepinephrine reuptake inhibitor
As above, serotonin-norepinephrine reuptake inhibitors (SNRI) duloxetine and venlafaxine are recommended in some medical guidelines as first-line or second-line therapy for DPN. A systematic review and meta-analysis of randomized controlled trials concluded there was evidence of moderate quality that duloxetine and venlafaxine each benefited greatly in reducing diabetic neuropathic pain. Common side effects include dizziness, nausea, and drowsiness.
Selective serotonin reuptake inhibitor
SSRIs including fluoxetine, paroxetine, sertraline, and citalopram have been found to be no more efficacious than placebo in several controlled trials and are therefore not recommended to treat painful diabetic neuropathy. Side effects are rarely serious and do not cause permanent disability. They cause sedation and weight, which can exacerbate the glycemic control of a person's diabetes. They can be used at doses that also alleviate the symptoms of depression, common comorbidity of diabetic neuropathy.
Tricyclic antidepressants
TCAs include imipramine, amitriptyline, desipramine, and nortriptyline. They are generally regarded as first-line or second-line treatment for DPN. From TCA, imipramine has been best studied. These medications effectively relieve pain symptoms but suffer from some dose-dependent side effects. One of the most important side effects is cardiac toxicity, which can cause a fatal abnormal heart rhythm. Other common side effects include dry mouth, sleeplessness, and sedation. At low doses used for neuropathy, toxicity is rare, but if symptoms require a higher dose, complications are more common. Among TCAs, amitriptyline is most widely used for this condition, but desipramine and nortriptyline have fewer side effects.
Opioid
Typical opioid drugs, such as oxycodone, appear to be no more effective than placebo. In contrast, low-quality evidence supports moderate benefits from the use of atypical opioids (eg, tramadol and tapentadol), which also have SNRI properties. Opioid drugs are recommended as second or third line treatment for DPN.
Topical agents
Capsaicin applied to the skin in 0.075% concentration has not been found to be more effective than placebo to treat pain associated with diabetic neuropathy. There is insufficient evidence to draw conclusions for a more concentrated form of capsaicin, clonidine, or lidocaine in the skin.
More
Low quality evidence supports a moderate beneficial effect of botulinum toxin injection. Dextromethorphan appears to be ineffective in treating diabetic neuropathic pain. There is not enough evidence to draw firm conclusions for the usefulness of nabone and nabiximol cannabinoids. There are several in vitro studies that show the beneficial effects of erythropoietin in diabetic neuropathy; However, one study of nerve conduction in individuals with mild-moderate diabetes suggests that erythropoietin alone or in combination with gabapentin has no beneficial effect on the development of diabetic neuropathy.
Medical devices
Monochromatic infrared photo energy therapy (MIRE) has been shown to be an effective therapy in reducing and often eliminating the pain associated with diabetic neuropathy. The studied wavelength of 890 nm is able to penetrate into the subcutaneous tissue where it acts on a special part of a cell called cytochrome C. Infrared light energy calls for Cytochrome C to release nitric oxide into the cell. Nitric oxide in turn promotes vasodilation which results in an increase in blood flow that helps nourish damaged nerve cells. Having nutrient-rich blood can reach the affected area (usually legs, lower legs and hands) it promotes regeneration of the neural tissues and helps reduce inflammation thereby reducing and/or relieving pain in the area.
Physical therapy
Physical therapy can help reduce reliance on painkiller therapy. Certain physiotherapy techniques can help relieve the symptoms that arise from diabetic neuropathy such as deep pain in the legs and feet, tingling or burning in the extremities, muscle cramps, muscle weakness, sexual dysfunction, and diabetic feet.
Transcutaneous electrical nerve stimulation (TENS) and interferential flow (IFC) use painless electrical currents and the physiological effects of low-frequency electrical stimulation to relieve stiffness, improve mobility, relieve neuropathic pain, reduce edema, and cure assistant foot ulcers.
Gait training, posture training, and teaching these patients the basic principles of off-loading can help prevent and/or stabilize foot complications such as foot ulcers. Off-loading techniques may include the use of mobility aids (eg crutches) or foot splints. Retraining gait will also be beneficial for individuals who have lost limbs, due to diabetic neuropathy, and are now using prosthesis.
The exercise program, along with manual therapy, will help prevent muscle contractures, seizures and atrophy. These programs may include general muscle stretching to maintain muscle length and range of motion. Common muscle strengthening exercises will help maintain muscle strength and reduce muscle wastage. Aerobic exercise such as swimming and using stationary bikes can help peripheral neuropathy, but activities that excessive pressure on the feet (eg walking away, running) may be contraindicated.
Heat, therapeutic ultrasound, hot wax is also useful for treating diabetic neuropathy. Pelvic floor muscle exercises can increase sexual dysfunction caused by neuropathy.
Strict glucose control
Treatment of early manifestations of sensorimotor polaruropathy involves an increase in glycemic control. The tight control of blood glucose can reverse the change of diabetic neuropathy, but only if new neuropathy and diabetes occur. In contrast, the symptoms of neuropathic pain in uncontrolled diabetics tend to subside as the disease develops and numbs.

Prognosis
The mechanism of diabetic neuropathy is poorly understood. Currently, treatment relieves pain and can control some related symptoms, but the process is generally progressive.
As a complication, there is an increased risk of leg injury due to loss of sensation (see diabetic foot). Small infections may develop into ulceration and this may require amputation.

Epidemiology
Diabetic neuropathy globally affects about 132 million people in 2010 (1.9% of the population).
Diabetes is the leading cause of neuropathy in the developed world, and neuropathy is the most common complication and the greatest source of morbidity and mortality in diabetes. It is estimated that neuropathy affects 25% of diabetics. Diabetic neuropathy is involved in 50-75% nontraumatic amputation.
The main risk factor for diabetic neuropathy is hyperglycemia. In the DCCT (Diabetes Control and Complications Trial, 1995) study, the annual incidence of neuropathy is 2% per year but drops to 0.56% with intensive type 1 diabetes. The development of neuropathy depends on the level of glycemic control in Type 1 and Type 2 diabetes. Duration of diabetes, age, smoking, hypertension, height, and hyperlipidaemia are also risk factors for diabetic neuropathy.

References
Further reading
-
Bril, Vera; English, John D.; Franklin, Gary M.; Backonja, Miroslav; Cohen, Jeffrey A.; Del Toro, David R.; Feldman, Eva L.; Iverson, Donald J.; Perkins, Bruce; Russell, James W.; Zochodne, Douglas W. (June 2011). "Evidence-based guidelines: Treatment of painful diabetic neuropathy reports from the American Association of Neuromuscular and Electrodiagnostic Medicine, the American Academy of Neurology, and the American Academy of Physical Medicine & Rehabilitation". Muscle & amp; Nerves . 43 (6): 910-917. doi: 10.1002/mus.22092. PMC 3100130 . PMID 21484835. - Pop-Busui, Rodica; Boulton, Andrew J.M.; Feldman, Eva L.; Bril, Vera; Freeman, Roy; Malik, Rayaz A.; Sosenko, Jay M.; Ziegler, Dan (December 20, 2016). "Diabetic Neuropathy: Position Statement by the American Diabetes Association". Diabetes Treatment . 40 (1): 136-154. doi: 10.2337/dc16-2042.

External links
- Diabetic Neuropathy in WebMD
- Diabetic Polyneuropathy at Medscape
- Diabetic Neuropathy at Diabetes.co.uk
- Diabetes Nerve Problems. Extensive MedlinePlus reference list of pertinent sites.
Source of the article : Wikipedia
